Features
Summary
Findings
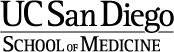
The left image shows a normal view of the esophagus and stomach. Compare the normal appearing GE (gastro-esophageal) junction with the image on the right. The right image shows an ill-defined, ulcerated lesion with irregular borders that has destroyed the normal architecture of the GE junction.
Impression
Gastric Carcinoma
Clinical Pathologic Correlation
The majority of stomach cancers (90-95%) are adenocarcinomas. Risk factors include chronic H. pylori infection (5-6x risk), smoking, diet (nitrosamines), autoimmune gastritis causing chronic inflammation, and possibly genetics. 50-60% occur in the pylorus and antrum. Patients are often asymptomatic until advanced disease. It is an aggressive tumor that spreads locally, and often metastasizes to lymph nodes and organs such as the ovaries and liver.
Pathology Pointer
Metastasis to various locations include the following: Virchow’s node-supraclavicular node; Krukenberg’s tumor – bilateral ovaries (showing “signet-ring” cells); Sister Mary Joseph nodule – periumbilical subcutaneous region
Preparation
Fresh
View
Gross photograph
Specimen
Esophagus and Stomach
Image Credit
Nissi Varki, M.D.Department of Pathology
School of Medicine
University of California, San Diego